Jusqu'à 40% de Réduction
Jusqu'à 30% de Réduction
Jusqu'à 40% de Réduction



Produit en promo


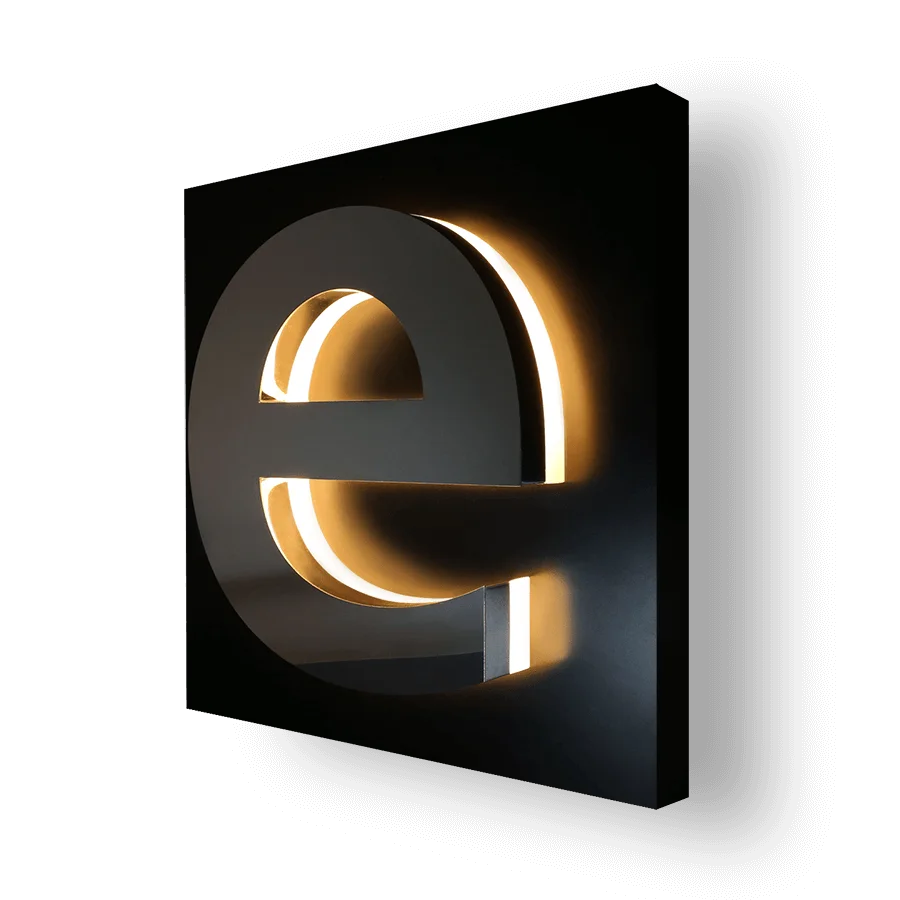
Logo Lumineuse finition Miroir
À partir de 990,00 DH
Croix de pharmacie double face
À partir de 2.790,00 DHProduits populaires aujourd'hui
-
Bâche, Signalétique, Tous les produits
Bâche agence immobilière
Bâche pour agence immobilière – Banderole à vendre à louer
Renouvelez vos supports de communication pour la vente ou la location de biens grâce à des bâches “à vendre”, “à louer” ultra design, claires et efficaces ! Nos bâches agence immobilière de 440g sont légères et résistantes aux intempéries, ce qui en font des panneaux immobiliers souples qui dureront dans le temps et pourront être réutilisés ! Plus pratique qu’un panneau rigide, vous pourrez transporter facilement vos bâches enroulables à vendre, vendu ou à louer : que vous soyez à pieds, dans les transports en commun ou en deux roues, vous pourrez emmener vos panneaux à vendre partout avec vous. Plusieurs formats disponibles.
SKU: n/a -
-
-
-
-
-
-
-
-
Administratif, Publicité / Commercial, Publicité / Commercial, Signalétique, Tous les produits
PLAQUES PROFESSIONNELLES IMPRIMÉES
 Administratif, Publicité / Commercial, Publicité / Commercial, Signalétique, Tous les produits
Administratif, Publicité / Commercial, Publicité / Commercial, Signalétique, Tous les produitsPLAQUES PROFESSIONNELLES IMPRIMÉES
Le PMMA est traité anti UV ce qui augmente la durée de vie du produit. L’utilisation du PMMA coulé permet une meilleure résistance à la coupe et à la casse.
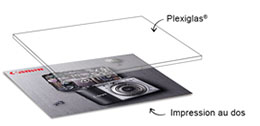
Votre visuel sera imprimé en vitrophanie au verso.
SKU: n/a -
-
-








 Eclairage : LED homogène, puissant et sans ombre.
Eclairage : LED homogène, puissant et sans ombre.
 Eclairage : LED homogène, puissant et sans ombre.
Eclairage : LED homogène, puissant et sans ombre.